
Geometries have always played a predominant ‘regulative’ role in human reasoning. The triangle was justifiably considered the most stable of geometric shapes by the ancients. The Egyptians chose it as the basis for their pyramids.The Buddhists found the circle to be the most logical shape and thus their metaphysics and the consequent sacred architectures are all based on the circle. Spinoza following Descartes would write his ‘Ethics’ based on geometric relations. Plato forbid those without knowledge of geometry from his academy.
In modern times no configuration has captured the human imagination more steadfastly than the double helix. Watson and Crick in their book by the same name attribute a great share of their discovery to playing with plastic models during lunch breaks [ to the chagrin of those who considered the scientific method as the only best way of discovery] that led to most celebrated of architectonics : the double helix as the crux behind Darwin’s ‘blind process’.
The ‘triple bottom line’ for healthcare is suggested to be Patient Experience , Cost and Population Health. The way that was arrived at is not spelt out. It is however clear that Berwick and Nolan equate ‘Patient Experience’ with ‘Quality’. But from a theory- building point – of- view there is a need for ‘ cognitive rearrangements ‘ in order to build a ‘stable architectonic’ for improvement science.

For this purpose, their model must be seen as an attempt to map the interrelationship between two global entities: healthcare system and society or in domain- specific terms between ‘quality of care’ and ‘quality of life’ . One of the earliest attempts at a ‘ Meta Systemic’ understanding of the health system is by Kerr White’s ‘ descriptive’ systemic analysis of how populations interact with the health system , well known as the ‘Ecology of Medical Care’ first proposed in 1961, updated in 2011 and 2016.
Russel Ackoff , in the system thinking literature provided a different ‘organisational design’ that is multidimensional. They distinguished the various components of their system as ‘input units’[function], output units [concerned with the direct production of value ] and the market units [ the management of expectation]. The triple aim erases the distinction between outside-in and inside-out perspectives because of its multidimensionality as it is a ‘mixture of different spaces’ eg individual and population.
Using micro economics as a guiding framework , we have since 2010 offered a framework of analysis that can be used especially in the developing countries , where there is a weak legacy of quality institutions and public policy, as the demand and supply equation of quality production. Building on this core we have extended the modular but dialectic model of improvement capability :
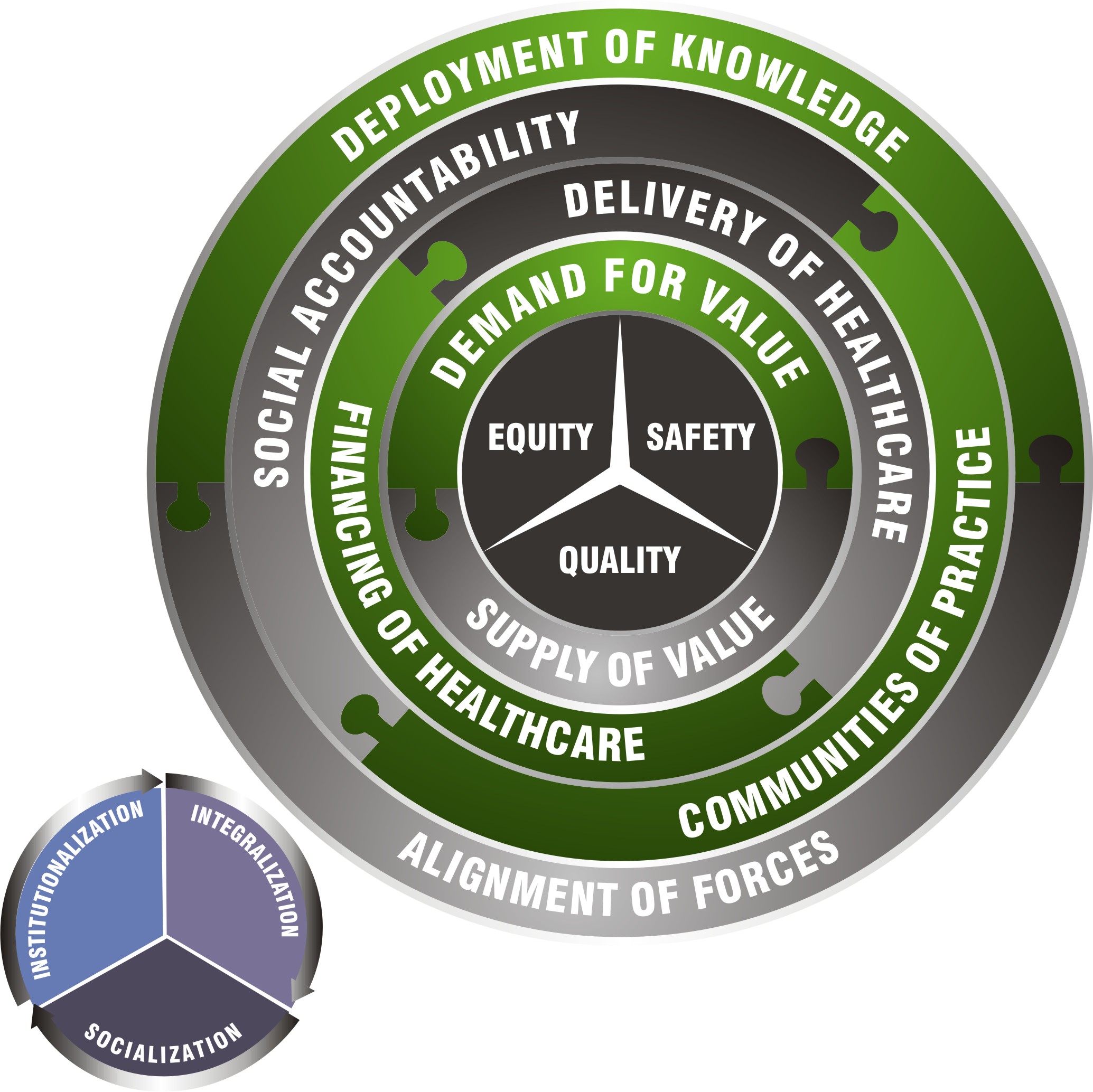
Don Berwick following Batalden’s introduction of microsystem theory, added the macro emphasis by proposing a ‘ chain of effects ‘. In that spirit, Berwick and Nolan introduced a ‘ system of effects’ by configuring a ‘ balanced’ ‘ policy compass’ for the healthcare system: Patient Experience, Cost and Population Health.
We always sought to make a distinction between micro-effectiveness and macro-effectiveness [just as in economics there is a distinction between micro economics and macro economics ]. It is in keeping with this ‘ functional’ delimitation that we offer the double helix to meaningfully locate the triple aim. However, the micro -macro distinction is not un-problematic even in economics: ‘on the one hand ‘ there are theorists who claim that all of economics is only macro-economics , citing the origins of the field as political economy and ‘on the other hand’ there are those that insist there is nothing called macroeconomics but only microeconomics that addresses macro problems. Don Berwick’s ‘chain of effects’ fortunately offers a ‘methodological vector’ for improvement science.
However, a mere super imposition of the ‘double helix’ to the ‘triad’ will produce a anomalous model. Thus there is a need for theoretical rearrangements and it may be acknowledged as a theoretical innovation, to offer a clear and distinct ‘ meta-system of effectiveness’ or a model of meta-effectiveness.
The first step to clarify the triple aim is to make a distinction between patient experience and quality . Even though it is not stated , it is likely that Berwick et al are ‘ over emphasizing ‘ the voice of the customer’ and under emphasizing the ‘voice of the professions’. This skewness has resulted in reactionary extensions of the idea of the triple aim into an Quadruple Aim: Patient Experience , Cost , Population Health and Professional Experience. Nevertheless, our approach is not to merely add ‘ effects’ to the model nor do we restrict professional experience to quality-of-worklife.

To do this we begin by pointing out the distinction between ‘patient experience’ and ‘ quality’ as the ‘modes of analysis’ and the ‘ modes of production’ still remain different due to the asymmetry of information and the ‘absoluteness of the other’ [ Levinas] that makes total ‘ co-production’ and total ‘ empathy’ merely ideals that cannot be reached in reality. Keeping in view this ‘predicament of inter-subjectivity ‘ we had in 2010 introduced a distinction between ‘clinical quality ‘ and a new domain called ‘ proximal quality’.
Proximal quality may be seen as the equivalent of patient centeredness and as a close approximation of ‘patient experience’ or the ‘phenomenology of care quality’. One could easily visualize the need for this distinction if we accept the possibility of two different perspectives: ‘first person’ non- empirical , subjective [ experience] perspective in proximal quality and the empirical , objective, ‘second person’ perspective in clinical quality. While both are at the bedside they are different in perspective : patient experience and professional experience. A theoretical vestige of the historical verstehen [understanding] vs erklaren[explanation] debate that gave rise to the Humanities.
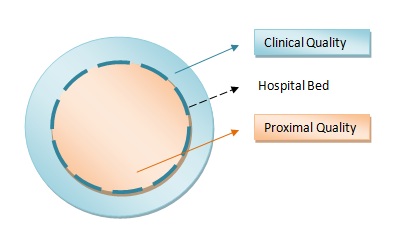
The demarcating ‘Thing’ is the ‘ hospital bed ‘ that serves as a two way glass. [ over-emphasizing the patient experience would merely call for the ‘inversion of pyramid’ metaphor]. The experience of care is perceived from the patient side of the bed and the clinical from the ‘ clinical professionals’ side. This distinction does not negate the possibility of empathy but instead provides a more realistic locus-standi for it.
The underlying pattern of power is that the patient is justified only in ‘demanding’ his own need [ for care] alone. Empowerment of the patient remains individual and personal. A lack of clarity is the root cause of violence against doctors and other care givers in Indian cities, when clinical outcomes are tragic. Proximal [ meaning close to the centre] Quality as a new ‘category’ acknowledges that patients always expect something more than clinical effects. The triple aim walks the extra mile by including the ‘population’ and ‘ health’ in the framework, but does not provide its own ‘grounding’. If the triple aim is the miraculous ‘skyhook’, the chain of effects is the ‘crane’. In the natural sciences, causes are limited to ‘Material’ and ‘Efficient’ causes of Aristotle, but anthropomorphic science like Improvement can accomodate Final[triple aim] and Formal[chain of effects] causes.
The second theoretical maneuver we suggest is to re-allocate the effects to individuals and populations. This requirement is unique to healthcare as its knowledge bases are divided between the clinical and community. The triple aim itself is a response to Kerr White’s call to build bridges between clinical medicine and public health. It is not a economic bridge[though it includes cost it is in reality a call for ‘systemic accountability’ for cost] but a ethical bridge. It has, once and for all, moved the ‘moral basis’ for healthcare beyond the individualistic, ‘principlistic’ ethical theories of Beuchamp and Childress . While there have been scholars of public health ethics, there have been no attempts to locate it in universal clinical practice. Don Berwick’s ‘chain of effects’ offers the metaphysical grounding for this ethics and thus constitutes the ‘DNA of Improvement’.
The lens of the double- helix framework identifies the ‘ problematics’ for improvement science to work in the future .
- How do patient experience [ proximal quality ] and professional experience [ clinical quality ] interact? We need to recognize that their ontologies are different.
- How does cost and quality relate to each other? Their constituencies are mostly different.
- What are the trade-offs in managing quality for the individual and the population. Their require different capabilities.
Micro effectiveness is human- relational will macro-effectiveness is social- control driven. Manufacturing industries do not make such distinctions as their theories preserve a clear distinction between production and market. A simple ‘summation of effects’ across the micro- macro chain over the ‘meso-systemic givens’, may not be statistically possible. Like micro economics and macro economics we need micro effectiveness and macro effectiveness. But how do these ‘ epistemics’ relate. While the proximal and clinical aspects of quality are determined at the individual level, the professional experience and cost are better leveraged by methodologies at the population level. They criss-cross or involve ‘chiastic reasoning’.
The construct validity for triple aim is usually articulated as overcoming the ‘ unbalanced ‘ goals or as creating a composite measure of public health quality. This idea of the stability of aims is the culmination of tradition including Batalden and Eugene Nelson’s clinical compass and the use of Kaplan’s balanced score card. Quality improvement methodology thus holds together the individual and population perspective without collapsing one into the other. The triple aim is a game changer. But these are not the reasons why the triple aim works. Does it provide the loftiest roof or the firmest floor. My argument is that it does both. The Triple Aim achieves the latter by, for the first time in the history of ideas in healthcare, ‘grounding’ three ‘ideal’ ‘systemic accountabilities’ in the ‘subject’ of every healthcare agent. There is ‘no system without an aim’, there is no aim without the ‘subject’. One could even see the ‘triple aim’ as a means of achieving the ‘chain of effects’.[not merely the vice versa]
Often times such initiatives are introduced on a ‘programmatic mode’: If we do this we can leverage healthcare effectiveness. In the western world, philanthropic and government funding is available for such initiatives, not merely because they do more good than harm,. but embody the ideals of ‘greater good’. Yet, the triple aim is not available to all eg developing countries , for the same reason. To become available universally requires theoretical justification that is more than strategic. Berwick et al over the years have offered not just boldness but subtlety to their ideas, subtlety to profoundness. This is missing in the next generation and I include myself in that criticism. In attempting to theorize I have no option but to problematise.
The descriptive maneuver of ‘labeling’ a set of aims as the ‘triple aim’ shouldn’t be the only claim as a ‘therapeutic’ theoretical construct. But what epistemic work does the triple aim do ?[ more specifically what more or what different epistemic work, as the concept of health maintenance have always been defined by these terms and Brent James has championed these outcomes at LDS since the early 90’s]. Are they without any externalities or are they without sub-optimization effects? Is the triple aim a short hand for the IOM six dimensions of quality? Further, it must guard against inadvertently imposing a ‘hierarchy of effects’: what is included in the triple aim are ‘ primary aims’ and what is excluded are the ‘secondary aims’. In this article, I bring into focus what is included merely by looking at their complements , if these where to be considered as ‘base pairs’. They are so indispensable to each other to the extent that they may be defined by the matched ‘other’. This is merely a call for a ‘ deeper balance’. Pragmatic, avante-garde cherry-picking of effects may lead to exclusions that are not justified theoretically: Aims will define the system and thus have immense power in shaping future healthcare. The triple aim is a theory about the future. [ and the future is always only in theory]
Unlike the triangular description [ or prescription] of the triple aim that is by definition limited, the geometry of the helix allows re-configurations and replications. It is not proposed that the relation between the two sets is a cause- effect relationship, even though it will be difficult to visualize the triple aim’s effectiveness without the other aims. I chose geometry to begin this post, as geometry is a non- causal science. The triple aim remains an efficient configuration of ‘universally’ desirable outcomes. It seeks to ‘formulate’ the ‘modal’ essence of healthcare improvement.
The ‘double helix effects’ does not diminish the triple aim but allows other triple aims to emerge in competition or collaboration : Organisations may constitute ‘replica’ triple aims as Quality, Cost and Family’s health. Professional bodies may pursue Quality, Professional Development and Individual Health. Such sub- systemic aims legitimately co- exist in the same moral economy of aims. It is Berwick’s ‘chain of effects’ that is required to bring them into play , hopefully through a helical structure, if the thesis of this post is right.
It is customary in science to describe relationships using ‘chain of causes’ , but systems thinking is itself a ‘post-structuralist’ idea and the ‘chain of effects’ is eminently acceptable as the template of improvement. We haven’t come across any theoretization of the idea and have thus dedicated this post to contribute our bit. The idea of ‘chain of causes’ and ‘analysis’ [which Ackoff would famously contrast with synthesis] have their sources in Descartes. Peirce would later suggest a ‘cable’ rather than ‘chain’ as a appropriate metaphor for epistemology: an idea not far from the helix.
The ‘triple aim’ has pride of place among many calls for a new social contract between the healthcare system and society: preserving the commitments to care, reducing ‘burden of illness’ and avoiding systemic waste. However, the aims of improvement science as a discipline will always be wider than the ‘equilibrium between aims’. The purpose of this post was to recover the conceptual coherence that may not be available through the triple aim, if seen in isolation. Ideas of ‘balance’ or ‘equilibrium’ are a-historical and do not include the parameter of ‘Time’. Changing the system by changing the aim is not without risk. It must be understood in the background of a ‘chain of effects’. How the triple aim can otherwise become available for those without funds is still a open question.
Developing countries , in the eagerness to join the bandwagon of big ideas, will adopt the triple aim. My worry is that they shouldn’t, like Feynman’s cult scientist hope for ‘goods’ to fall from the sky. The map is not the territory. The scorecard is not the game. To pursue ‘Universal Coverage’, they must first learn to navigate the ‘chain of effects’ which has a rich history of technical and policy innovations, spread over several decades. As Hegel reminded us the ‘owl of Minerva spreads its wings only with the falling of dusk’.
Note: This post is not so much about ‘methodology’ but instead demonstrates the usefulness of ‘history of ideas’ [in general and healthcare in specific] to the future development of improvement as a ‘rigorous’ science.
I have not attempted an exegetical analysis of Berwick et al 2008 paper, as it is offered as a policy note for the US Healthcare System and thus makes several ‘institutional assumptions’. While they emphasize the empirical ‘necessities’ for vertical and horizontal integration in healthcare, I have taken a step back to look at the ‘aim’ of the triple aim: to locate the triple aim in Modal [necessities and possibilities; CI Lewis was a pioneer of modal logic and possible world theories] and Moral discourse. My intention is to develop it as a pure or universal concept that hopefully goes beyond ’empirical constraints’.
In Plato’s dialogue ‘Meno’, Socrates uses a geometrical figure to demonstrate his ‘alethic’ or anamnestic theory of knowledge. I have borrowed geometry merely to chart an axiological cartography for improvement science. Exploratory Graphical analysis and visual thinking are ‘smart’ components of improvement methods. While Pierce is credited with introducing blinded,randomised trials [ before Fisher] and repeated measures analysis, he is also the first to introduce ‘figural reasoning’ through his ‘existential graphs’.
We often do not speak of the scientific method as being circular. This idea of circularity [in PDSA] is C I Lewis’s direct ‘textual’ influence on Walter Shewart. Peirce would in his late years change his middle name ‘sanders’ to ‘santiago’ as an expression of gratitude to William James for his unstinting support. In his letters to James, he would often refer to ‘ boodha’ [ Buddha] in the context of his own suffering . It would be difficult to argue against the ‘sub-textual’ influence of Buddhist epistemology on pragmaticism and the central ideas of improvement science.
1